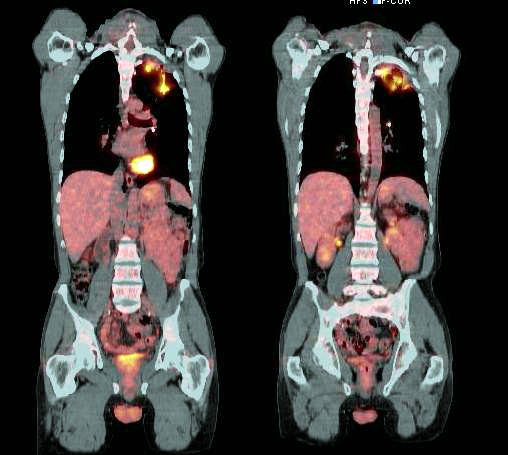
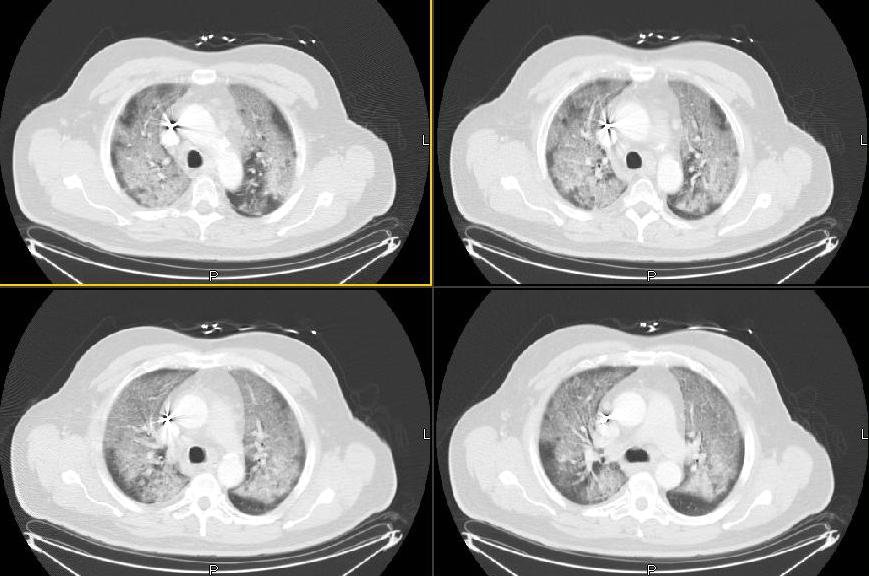
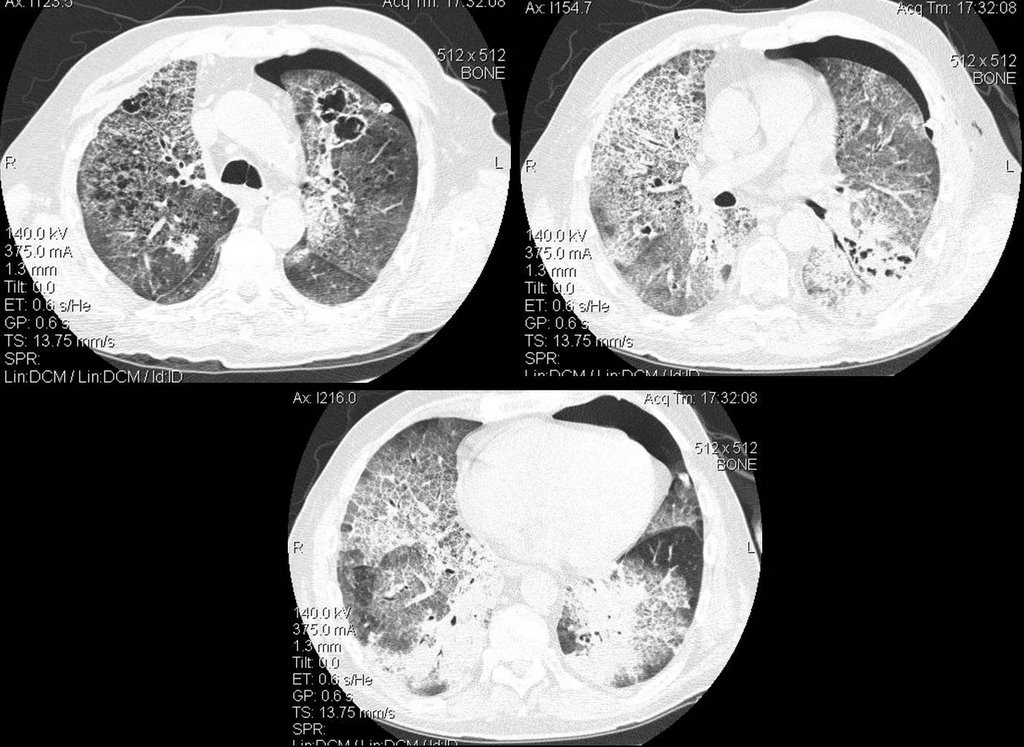
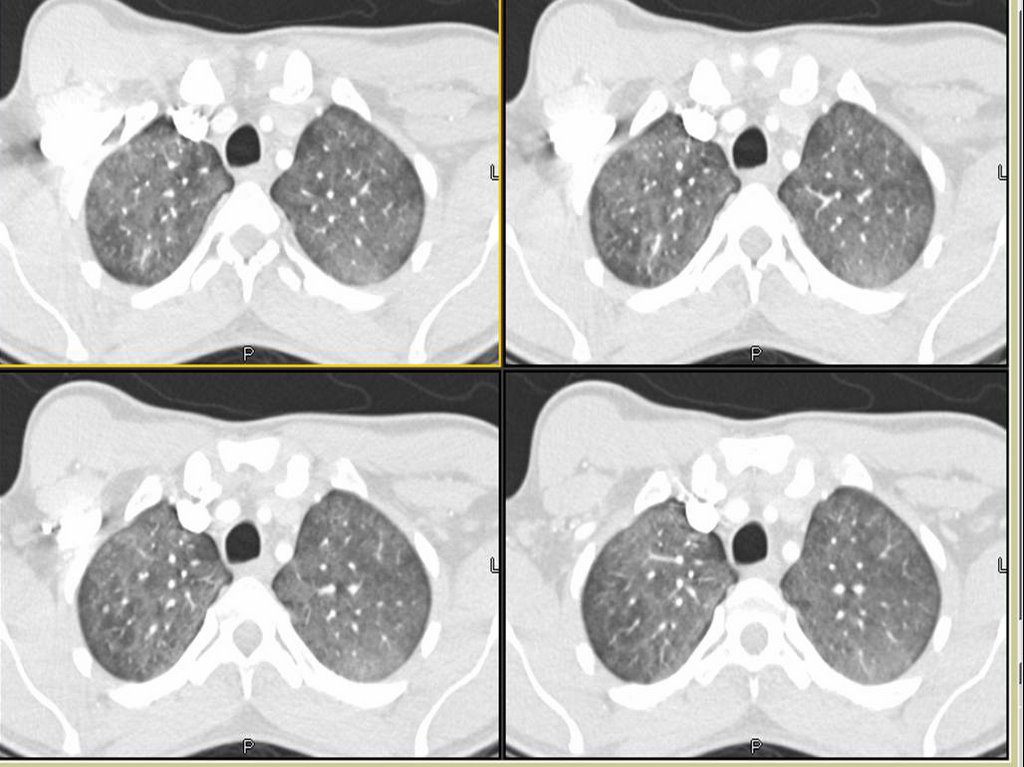
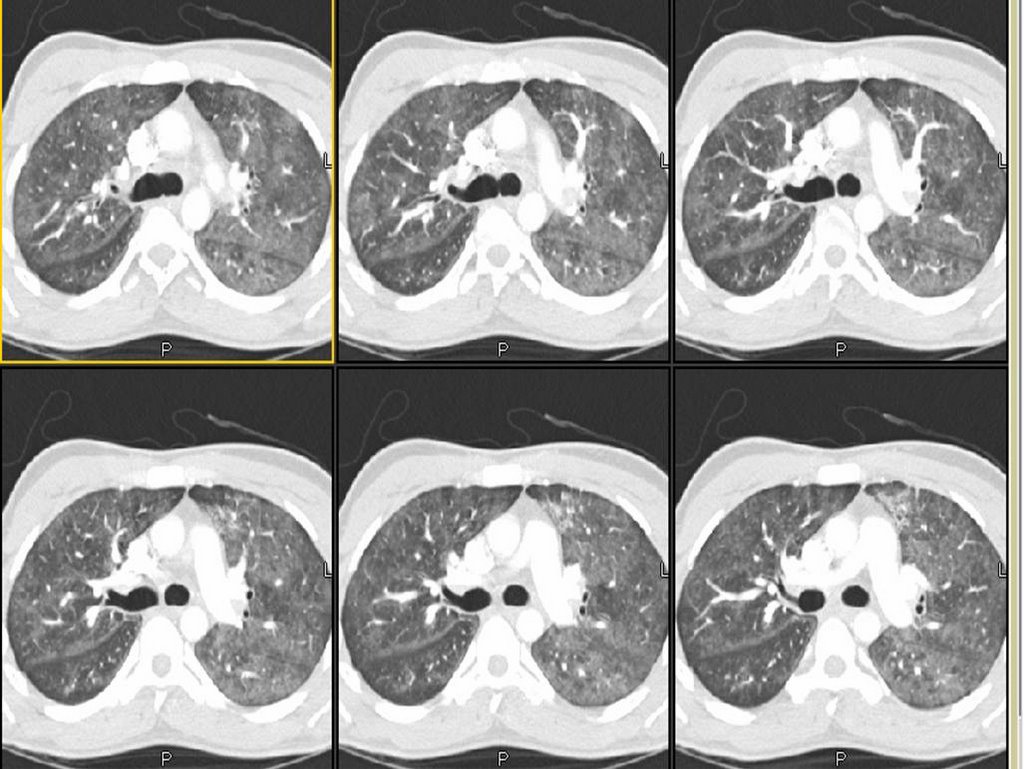
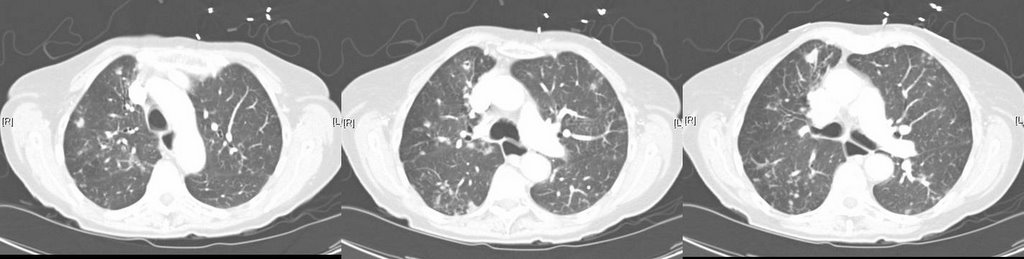
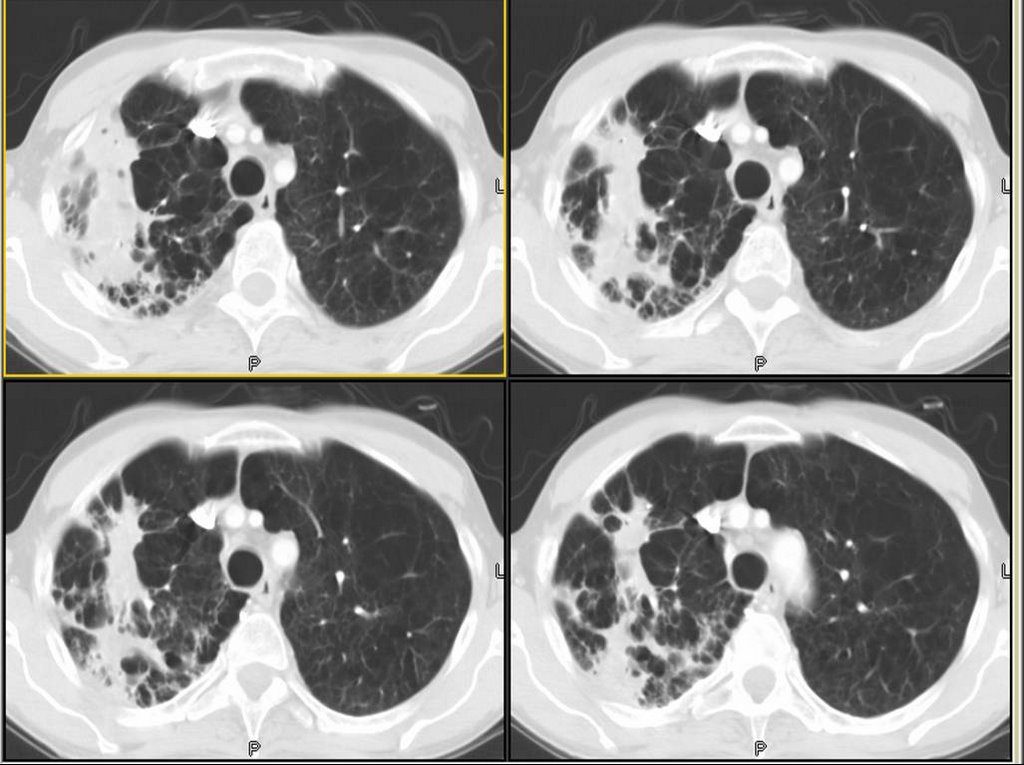
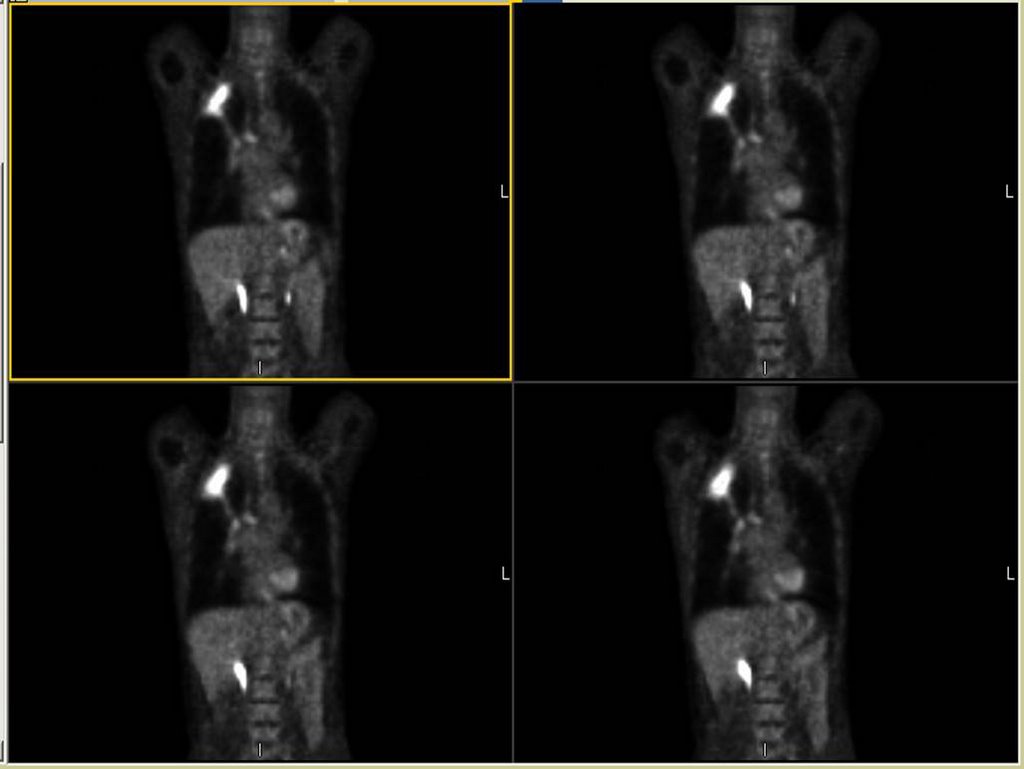
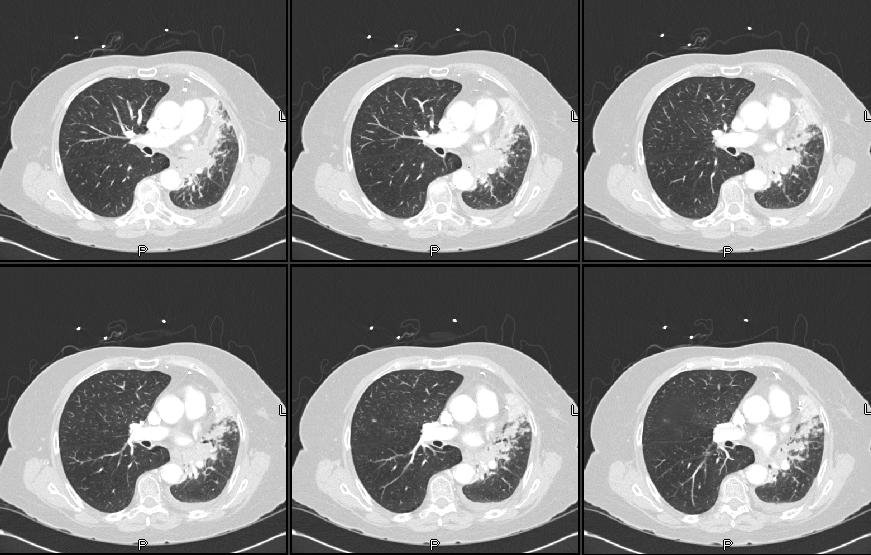
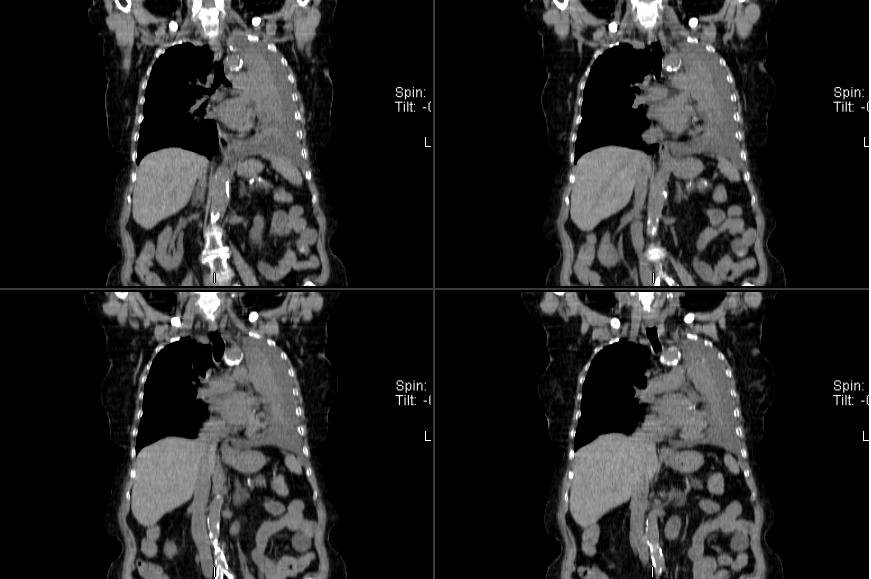
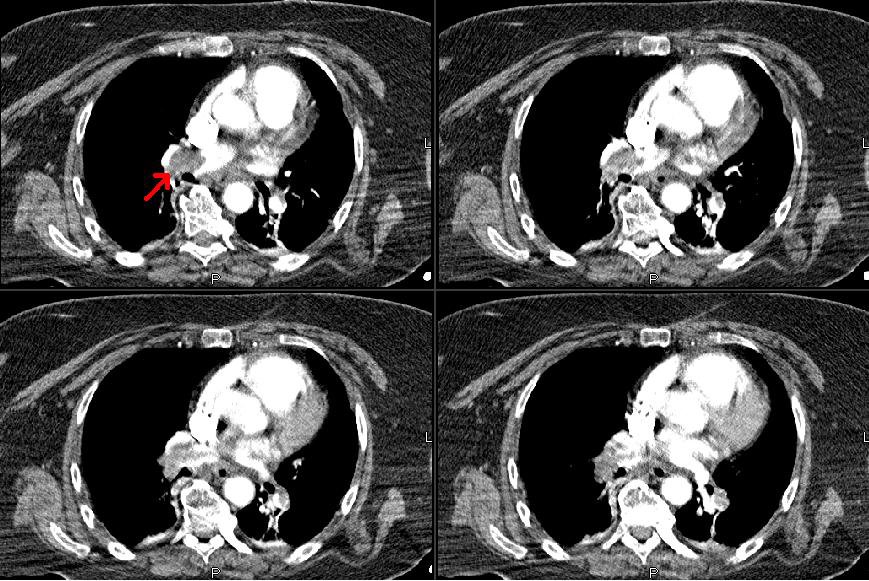
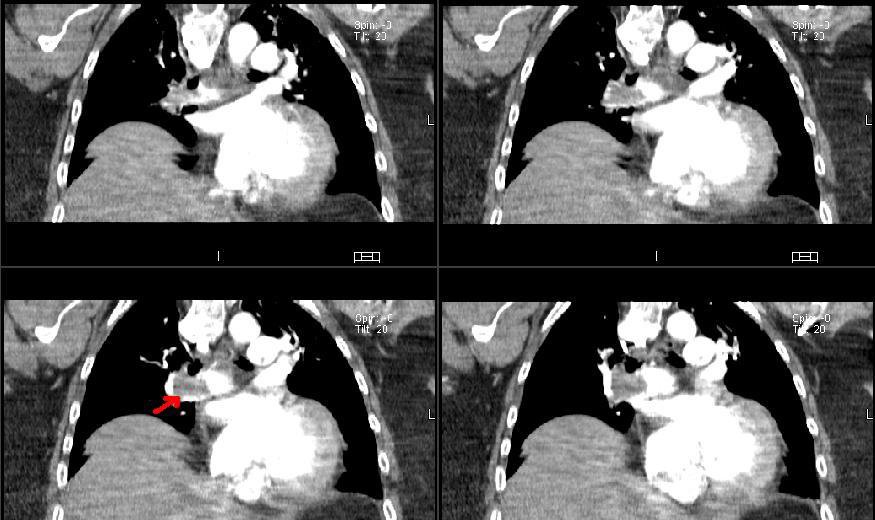
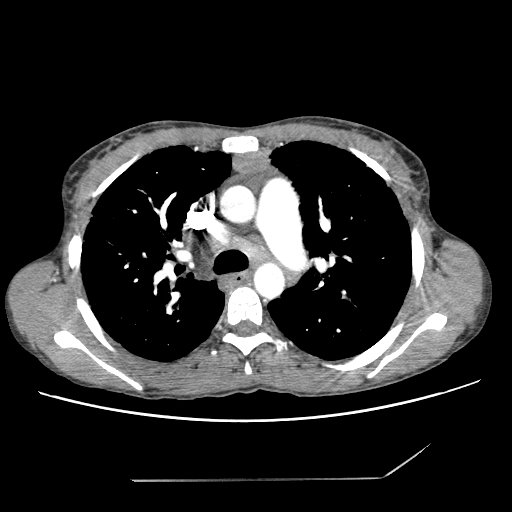
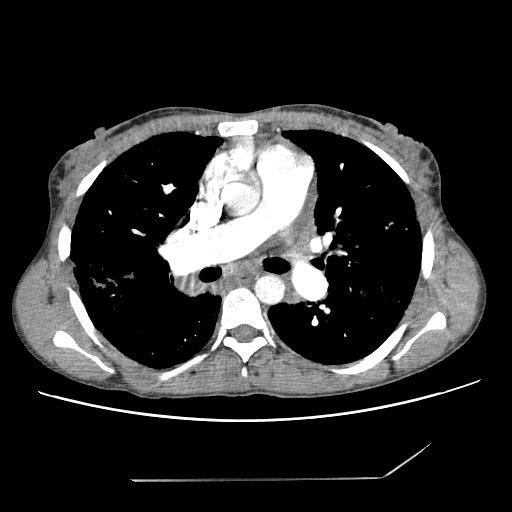
18-year-old male referred for hemoptysis. He reports several episodes of pneumonia in last several years. His mother believes that these have all been on the "right chest." The most recent episode of pneumonia had occurred during the last football season, when he developed cough and hemoptysis. By report, he had an abnormal chest x-ray at that time. He was treated with antibiotics and reports that the symptoms resolved. He again had hemoptysis in a few months later. A PPD was negative. No images of a chest CT, but there was right middle lobe bronchiectasis.
Pmhx Status post hernia repair, rhinoplasty, right elbow surgery. In addition, the patient has a history of a racing heart and has been worked up for possible supraventricular tachycardia. In addition, the patient had a mole punch biopsied off his left back inferior to the scapula and does not know what the pathology for this showed.
SH: no alcohol, tobacco, or drug use
Physical Exam: His P is 49. BP is 108/57. His RR is 16, and his WT is 79 kg. In appearance, he is a well-developed, well- nourished young man in no distress. HEENT: Lymph node examination was no supraclavicular adenopathy. Pulmonary: clear to auscultation with both quiet and forced expiratory maneuvers from base to apex bilaterally. He is resonant to percussion throughout. Cardiac examination: Regular rhythm. S1 and S2 are of normal quality without murmur, gallop, or rub. He had no pedal edema, and he had 2+ radial pulses.
A bronch showd the following in the RML:

My collegue proceeded to evaluate further into the bronchus where they identified copious mucous and a
foreign body. The foreign body was extracted with biopsy forceps. Under direct visualization it appeared to be a piece of organic green matter that resembled a branch tip of a pine tree.
Final diagnosis:
LUNG, RIGHT MIDDLE LOBE, BIOPSY:
1. BENIGN MARKEDLY INFLAMED BRONCHIAL MUCOSA AND FRAGMENTS OF
GRANULATION TISSUE.
2. FOREIGN MATERIAL CONSISTENT WITH VEGETABLE PARTICLE.
B. RIGHT LOBE, BIOPSY: FOREIGN BODY.
The patient breathed in a pine needle....